|
Overview
 People think of a bunion as being as a bump on the side of the foot near the big toe. However, bunions go deeper than what we can see. Although the skin might be red, a bunion actually reflects a change in the anatomy of the foot. Bunions happen over time. What begins as the big toe pointing toward the second toe ends up as changes in the actual alignment of the bones in the foot. There is also a condition called tailor?s bunion or bunionette. This type of bump differs from a bunion in terms of the location. A tailor?s bunion is found near the base of the little toe on the outside of the foot. People think of a bunion as being as a bump on the side of the foot near the big toe. However, bunions go deeper than what we can see. Although the skin might be red, a bunion actually reflects a change in the anatomy of the foot. Bunions happen over time. What begins as the big toe pointing toward the second toe ends up as changes in the actual alignment of the bones in the foot. There is also a condition called tailor?s bunion or bunionette. This type of bump differs from a bunion in terms of the location. A tailor?s bunion is found near the base of the little toe on the outside of the foot.Causes Bunions are caused by pressure on the inside of the forefoot which causes the 1st metatarsal bone in the foot to migrating outwards. Biomechanical factors can contribute to the development of bunions for example if you over pronate where the foot rolls in or flattens excessively which causes the inside of the foot to rub against the shoe. Wearing high heeled shoes regularly also increases the risk of developing the condition . The pressure on the forefoot is increased considerably as the heel is raised up. Age is also a factor as the ligaments lose strength as you get older. Symptoms With Bunions, a person will have inflammation, swelling, and soreness on the side surface of the big toe. Corns most commonly are tender cone-shaped patches of dry skin on the top or side of the toes. Calluses will appear on high-pressure points of the foot as thick hardened patches of skin. Diagnosis Your doctor will ask questions about your past health and carefully examine your toe and joint. Some of the questions might be: When did the bunions start? What activities or shoes make your bunions worse? Do any other joints hurt? The doctor will examine your toe and joint and check their range of motion. This is done while you are sitting and while you are standing so that the doctor can see the toe and joint at rest and while bearing weight. X-rays are often used to check for bone problems or to rule out other causes of pain and swelling. Other tests, such as blood tests or arthrocentesis (removal of fluid from a joint for testing), are sometimes done to check for other problems that can cause joint pain and swelling. These problems might include gout , rheumatoid arthritis , or joint infection. Non Surgical Treatment Wearing good footwear does not cure the deformity but may ease symptoms of pain and discomfort. Ideally, get footwear advice from a person qualified to diagnose and treat foot disorders (podiatrist - previously called a chiropodist). Advice may include wear shoes, trainers or slippers that fit well and are roomy. Don't wear high-heeled, pointed or tight shoes. You might find that shoes with laces or straps are best, as they can be adjusted to the width of your foot. Padding over the bunion may help, as may ice packs. Devices which help to straighten the toe (orthoses) are still occasionally recommended, although trials investigating their use have not found them much better than no treatment at all. Painkillers such as paracetamol or ibuprofen may ease any pain. If the bunion (hallux valgus) develops as part of an arthritis then other medication may be advised. A course of antibiotics may be needed if the skin and tissues over the deformity become infected.  Surgical Treatment Severe cases may require, along with surgery, cast immobilization and prolonged avoidance of weight-bearing activity. You should know that undergoing surgery for this health problem does not guarantee a cure or even a beneficial health outcome. Bunions, like many other foot conditions, should always be approached from a prevention standpoint, or therapy should be directed at slowing the progression of your deformity. Prevention Here are some tips to help you prevent bunions. Wear shoes that fit well. Use custom orthotic devices. Avoid shoes with small toe boxes and high heels. Exercise daily to keep the muscles of your feet and legs strong and healthy. Follow your doctor?s treatment and recovery instructions thoroughly. Unfortunately, if you suffer from bunions due to genetics, there may be nothing you can do to prevent them from occurring. Talk with your doctor about additional prevention steps you can take, especially if you are prone to them. Overview
Over-pronation describes a characteristic gait wherein a lack of sufficient support from the arch of the foot causes it to roll inwards as weight is placed on it. The long arch of the foot is actually a very important structure in terms of our gait and how we walk, it is responsible for ensuring that as our weight rolls from the heel to the balls of our feet it does so in a straight line that doesn?t place undue stress on the ankle or knees. Unfortunately when a person?s arch is not pronounced enough, or even simply not there (a condition called flat footedness), there isn?t enough arch support to maintain a healthy, forward motion of the foot.  Causes Congenital "Flat Feet" - an individual may be born with feet that lack an appropriately supportive arch thereby predisposing the individual to this foot condition. Excessive Weight (Obesity) Too much weight on the foot from either obesity or pregnancy may be a factor. Repetitive Impact walking on flat, hard surfaces continuously places unnatural stress on the foot arch. Symptoms Due to the laxity of the soft tissue structures of the foot, and the fact that the joints are not held together properly, the bones of the feet shift. When this occurs, the muscles that attach to these bones must also shift, or twist, in order to attach to these bones. The strongest and most important muscles that attach to our foot bones come from our lower leg. So, as these muscles course down the leg and across the ankle, they must twist to maintain their proper attachments in the foot. This twisting of these muscles will cause shin splints, Achilles Tendonitis, generalized tendonitis, fatigue, muscle aches and pains, cramps, ankle sprains, and loss of muscular efficiency (reducing walking and running speed and endurance). The problems we see in the feet, which are due to over-pronation include bunions, heel spurs, plantar fasciitis, fallen and painful arches, hammertoes, metatarsalgia (ball of foot pain), and calluses. Diagnosis One of the easiest ways to determine if you overpronate is to look at the bottom of your shoes. Overpronation causes disproportionate wear on the inner side of the shoe. Another way to tell if you might overpronate is to have someone look at the back of your legs and feet, while you are standing. The Achilles tendon runs from the calf muscle to the heel bone, and is visible at the back of the ankle. Normally it runs in a straight line down to the heel. An indication of overpronation is if the tendon is angled to the outside of the foot, and the bone on the inner ankle appears to be more prominent than the outer anklebone. There might also be a bulge visible on the inside of the foot when standing normally. A third home diagnostic test is called the ?wet test?. Wet your foot and stand on a surface that will show an imprint, such as construction paper, or a sidewalk. You overpronate if the imprint shows a complete impression of your foot (as opposed to there being a space where your arch did not touch the ground).  Non Surgical Treatment Fortunately, there are simple things you can do to cure and correct your overpronation issues. Certain exercises help. Pull your toes back using a rolled up towel. Roll your feet over a golf or tennis ball for a minute. And do calf raises by standing up and lifting up on your toes. These all help reposition the foot and strengthen the muscles and tendons necessary for proper support. Beyond that, simple adjustments to footwear will help immensely. Surgical Treatment Subtalar Arthroereisis. Primary benefit is that yje surgery is minimally invasive and fully reversible. the primary risk is a high chance of device displacement, generally not tolerated in adults. An implant is pushed into the foot to block the excessive motion of the ankle bone. Generally only used in pediatric patients and in combination with other procedures, such as tendon lengthening. Reported removal rates vary from 38% - 100%, depending on manufacturer. Overview
Sever's disease is an overuse syndrome involving an immature part of the skeleton. Pain goes away when the overuse is over, or when the growing is done. Hence, the disease is self-limited, in that the pain goes away eventually when growth in the heel bone is complete at about age 13. Even if the child is hurting, as long as he can tolerate it, he may continue to take part in sports. No long term disability is expected from this problem. Causes With early puberty, the growth plate at the end of the heel develops, transforming cartilage cells into bone cells. This painful heel condition occurs during these growth spurts, when the heel bone grows more rapidly than the muscles and tendons of the leg. The discrepancy between rates of development causes excess pressure and tension to be placed upon the heel and it becomes less flexible. This condition affects active children the most. Due to the amount of exercise, more stress is placed upon the tendons which in turn causes more damage to the growth plate. The bone plates fully mature and harden by the time a child reaches the age of 15. Symptoms On examination, the typical signs are tenderness on palpation of the heel, particularly on deep palpation at the Achilles tendon insertion. Pain on dorsiflexion of the ankle, particularly when doing active toe raises; forced dorsiflexion of the ankle is also uncomfortable. Swelling of the heel, usually mild. Calcaneal enlargement, in long-standing cases. Diagnosis Your podiatrist will take a comprehensive medical history and perform a physical examination including a gait analysis. The assessment will include foot posture assessment, joint flexibility (or range of motion), biomechanical assessment of the foot, ankle and leg, foot and leg muscle strength testing, footwear assessment, school shoes and athletic footwear, gait analysis, to look for abnormalities in the way the feet move during gait, Pain provocation tests eg calcaneal squeeze test. X-rays are not usually required to diagnose Sever?s disease. Non Surgical Treatment A doctor, sports therapist or physiotherapist can apply a plaster cast or boot if the child is in severe pain. This may be worn for a few days or even weeks and should give relief of pain for a while. Carry out a full biomechanical assessment. This may help to determine if any foot biomechanics issues are contributing to the condition. Orthotics or insoles can be prescribed to help correct over pronation or other biomechanics issues. Prescribe anti-inflammatory medication such as ibuprofen to reduce pain and inflammation. This will not be prescribed if asthma the child has asthma. In persistent cases X-rays may be taken but this is not usual. A doctor, sports therapist or physiotherapist will NOT give a steroid injection or operate as these are not suitable treatment options. The condition will usually settle within 6 months, although it can persist for longer. Recovery This condition is self limiting, it will go away when the two parts of bony growth join together, this is natural. Unfortunately, Sever's disease can be very painful and limit sport activity of the child while waiting for it to go away, so treatment is often advised to help relieve it. In a few cases of Sever's disease, the treatment is not successful and these children will be restricted in their activity levels until the two growth areas join, usually around the age of 16 years. There are no known long term complications associated with Sever's disease.
Overview
 Achilles tendon rupture is most common in people aged 30-50. Patients may describe the injury as feeling or hearing a snap or bang, or as feeling they have been shot in the back of the leg. On examination, patients will have reduced plantarflexion and a positive Thompson test. Surgery is associated with a lower risk of re-rupture and a greater likelihood of returning to sporting activity. Conservative management reduces the chance of complications. Achilles tendon rupture is most common in people aged 30-50. Patients may describe the injury as feeling or hearing a snap or bang, or as feeling they have been shot in the back of the leg. On examination, patients will have reduced plantarflexion and a positive Thompson test. Surgery is associated with a lower risk of re-rupture and a greater likelihood of returning to sporting activity. Conservative management reduces the chance of complications.Causes Achilles tendon rupture occurs in people that engage in strenuous activity, who are usually sedentary and have weakened tendons, or in people who have had previous chronic injury to their Achilles tendons. Previous injury to the tendon can be caused by overuse, improper stretching habits, worn-out or improperly fitting shoes, or poor biomechanics (flat-feet). The risk of tendon rupture is also increased with the use of quinolone antibiotics (e.g. ciprofloxacin, Levaquin). Symptoms Patients with an Achilles tendon rupture frequently present with complaints of a sudden snap in the lower calf associated with acute, severe pain. The patient reports feeling like he or she has been shot, kicked, or cut in the back of the leg, which may result in an inability to ambulate further. A patient with Achilles tendon rupture will be unable to stand on his or her toes on the affected side. Diagnosis During the physical exam, your doctor will inspect your lower leg for tenderness and swelling. In many cases, doctors can feel a gap in your tendon if a complete rupture has occurred. The doctor may also ask you to kneel on a chair or lie on your stomach with your feet hanging over the end of the exam table. He or she may then squeeze your calf muscle to see if your foot will automatically flex. If it doesn't, you probably have ruptured your Achilles tendon. If there's a question about the extent of your Achilles tendon injury, whether it's completely or only partially ruptured, your doctor may order a magnetic resonance imaging (MRI) scan. This painless procedure uses radio waves and a strong magnetic field to create a computerized image of the tissues of your body. Non Surgical Treatment Once the Achilles tendon is partially damaged, one should exercise great care. The risk of rupture is high and if pain is associated with walking, one should consult with an orthopedic surgeon or a sports physician. A complete rupture of the Achilles tendon is never treated at home. It is important to understand that there are no minerals, nutrients, or herbs to treat Achilles tendon injury and any delay just worsens the recovery. 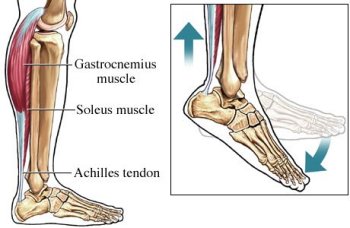 Surgical Treatment Operative treatment of Achilles tendon ruptures involves opening the skin and identifying the torn tendon. This is then sutured together to create a stable construct. This can be performed through a standard Achilles tendon repair technique or through a mini-incision technique (to read about the different types of techniques, look under ?Procedure? in Achilles Tendon Repair). By suturing the torn tendon ends together, they maintain continuity and can be mobilized more quickly. However, it is critical to understand that the return to normal activities must wait until adequate healing of the tendon has occurred. The potential advantages of an open repair of the Achilles tendon include, faster recovery, this means that patients will lose less strength. Early Range of Motion. They are able to move the ankle earlier so it is easier to regain motion. Lower Re-rupture Rate. The re-rupture rate may be significantly lower in operatively treated patients (2-5%) compared to patients treated non-operatively (8-15%). The main disadvantage of an open repair of the Achilles tendon rupture is the potential for a wound-healing problem which could lead to a deep infection that is difficult to eradicate, or a painful scar.
Overview
This condition is characterized by a progressive flattening or falling of the arch. It is often referred to as posterior tibial tendon dysfunction (PTTD) and is becoming a more commonly recognized foot problem. Since the condition develops over time, it is typically diagnosed in adulthood. It usually only develops in one foot although it can affect both. Since it is progressive, it is common for symptoms to worsen, especially when it is not treated early. The posterior tibial tendon attaches to the bones on the inside of your foot and is vital to the support structure within the foot. With PTTD, changes in the tendon impair its ability to function normally. The result is less support for the arch, which in turn causes it to fall or flatten. A flattening arch can cause the heel to shift out of alignment, the forefoot to rotate outward, the heel cord to tighten, and possible deformity of the foot. Common symptoms include pain along the inside of the ankle, swelling, an inward rolling of the ankle, pain that is worse with activity, and joint pain as arthritis sets in.  Causes Damage to the posterior tendon from overuse is the most common cause for adult acquired flatfoot. Running, walking, hiking, and climbing stairs are activities that add stress to this tendon, and this overuse can lead to damage. Obesity, previous ankle surgery or trauma, diabetes (Charcot foot), and rheumatoid arthritis are other common risk factors. Symptoms Initially, flatfoot deformity may not present with any symptoms. However, overtime as the tendon continues to function in an abnormal position, people with fallen arches will begin to have throbbing or sharp pain along the inside of the arch. Once the tendon and soft tissue around it elongates, there is no strengthening exercises or mechanism to shorten the tendon back to a normal position. Flatfoot can also occur in one or both feet. If the arch starts to slowly collapse in one foot and not the other, posterior tibial dysfunction (PTTD) is the most likely cause. People with flatfoot may only have pain with certain activities such as running or exercise in the early phase of PTTD. Pain may start from the arch and continue towards the inside part of the foot and ankle where the tendon courses from the leg. Redness, swelling and increased warmth may also occur. Later signs of PTTD include pain on the outside of the foot from the arch collapsing and impinging other joints. Arthritic symptoms such as painful, swollen joints in the foot and ankle may occur later as well due to the increased stress on the joints from working in an abnormal position for a long period of time. Diagnosis Examination by your foot and ankle specialist can confirm the diagnosis for most patients. An ultrasound exam performed in the office setting can evaluate the status of the posterior tibial tendon, the tendon which is primarily responsible for supporting the arch structure of the foot. Non surgical Treatment In the early stages, simple pre-fabricated orthotics can help improve the heel position to reduce the mechanical load which is contributing to the symptoms. In advanced stages or long term orthotic use, a plaster of paris or foam box cast can be taken and specific bespoke orthotics manufactured. If the condition develops further a AFO (ankle foot orthotic) may be necessary for greater control. In more advanced stages of symptomatic Adult Acquired flat feet, where the conservative methods of treatment have failed there are various forms of surgery available depending upon the root cause of the issue and severity.  Surgical Treatment Many operations are available for the treatment of dysfunction of the posterior tibial tendon after a thorough program of non-operative treatment has failed. The type of operation that is selected is determined by the age, weight, and level of activity of the patient as well as the extent of the deformity. The clinical stages outlined previously are a useful guide to operative care (Table I). In general, the clinician should perform the least invasive procedure that will decrease pain and improve function. One should consider the effects of each procedure, particularly those of arthrodesis, on the function of the rest of the foot and ankle. |
